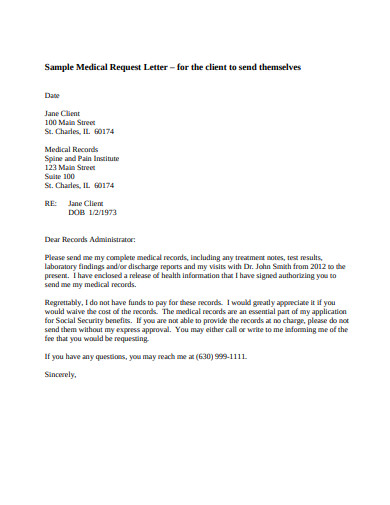
Salutations are added to address the person whom you are writing this letter. Change your GP practice.
 5 Medical Request Letter Templates In Pdf Doc Free Premium Templates
5 Medical Request Letter Templates In Pdf Doc Free Premium Templates
I am requesting approval to add my sondaughter Name.

Request medical card. You may be asked to provide evidence of your identity. In the meantime you still can receive healthcare services. Once youve completed the process the card.
You can also request that the information it contains be corrected if there is an error or if your situation changes. Otherwise use the form below to request invitation now. If you are making an access request to a HSE service pdf you can write to the health service or send it a HSE Subject Access Request.
If you have any questions about the form call us before you fill it out. Change your Surname. I thank you for your cooperation to this request.
If youre visiting a GP youve visited before they should already have you in the system. I am writing this letter in relation to my family medical card. If you require your medical card in another language please contact the BSO on the following number 0300 555 0113 where you will be advised on how to make your request.
What do I do if my Medical Card is lost or stolen. By providing your email address you consent to the Department contacting you through that email address. Finally you can call the Member Contact Center to request a card be mailed.
This is the quickest method of getting the card. If you dont have your ID card handy please call 1-866-414-1959 8 am - 10 pm ET Monday-Friday. The office should be able to give you your number.
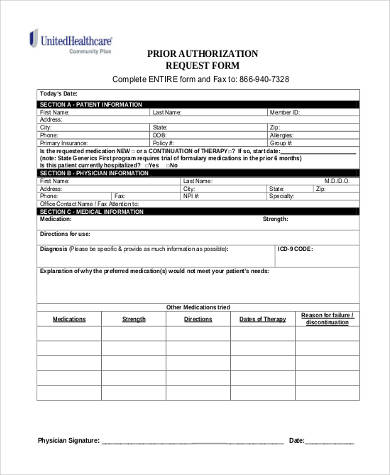
Access medical services prescription medicines and hospital care for free. Apply and renew online. The first section in a request letter to start with is the details of the receiver to whom you.
My family Medical Card details are as follows. Mr XXX PPS Number. This is an automated system and all requests will be processed in English.
A request for information from health medical records has to be made with the organisation that holds your health records the data controller. You can request to have a damaged lost or stolen card replaced. The card will take up to two weeks to arrive.
Employee cash advance form template has personal and contact information and bank and loan supervisor information. To access your information write to the relevant health service to make a data access request. Contact the GP whom you are registered with to apply for another card.
If this is a medical emergency please call 911. For hospital health records contact the records manager or patient services manager at the relevant hospital trust. If youve forgotten your NHS medical card number your general practitioner will be your best resource.
When calling choose option 5 to speak to a representative about ordering a replacement Health First Colorado card. If you already requested an invitation code open our first initial email message from the Care Clinic requesting your response and click the confirm link to re-process receiving your invitation. Forms HS200 and HSCR-1 are available at GP Practices.
Leave a line after the. Always take your picture ID with you. Fill out form GMS1.
Apply for a medical card. A new card can be issued if you. Post the completed form to the National Medical Card Unit PO Box 11745 Dublin 11 D11 XKF3.
Medical card application process. XXXXXX Copy of birth certificate attached onto my family Medical Card. Documents you need to include with your medical card application.
Download the form in English or Irish or LoCall 1890 252 919 to order one. You can get your new style medical card by applying on line at. Inform BSO directly of a Date of Birth error.
Replacing a lost NHS medical card is done by contacting either the GP you are registered with or the local health authority that covers your area. You can also call or go in person to your local County Department of Human Services to request a card be mailed. You can apply online for a medical card on medicalcardie.
His office will provide you with Form GMS1 the family doctor services registration form. XXXX Date of Birth. If you have any questions before you send your application you can phone Lo-call 1890 252 919 contact your Local Health Office or email clientregistrationhseie.
MEDICAL MARIJUANA CARD INVITATION. GPs who accept medical cards. There is no charge for a replacement card.
If you are continuing to see this message and need immediate assistance please call the number located on the back of your ID card. Change Replacement or Surrender Request Instructions In order to change replace or surrender your Medical Marijuana Use Registry Identification Card complete the Cardholder Information section and applicable sections of this form. Appeal a medical card decision.
Call DHS 1-800-843-6154 or HFS 1-800-226-0768 TTY 1-877-204-1012 to request a replacement card. However in some cases usually for security reasons you may be asked to provide identification to prove you are the person whose number you are requesting. A fee may apply.
Use this cash advance request form template for the employees or workers to submit their cash advanced request for their vacation personal or company travels and etc. Your replacement Medical Card will be mailed to you. For example your GP practice optician or dentist.
6 Steps to Write a Medical Request Letter Step 1. The procedure for replacing or correcting a card is the same for your child. To apply for a medical card by post.