You can print a blank CMS1500 Form from the Client Ledger. Blank Cms 1500 Form Printable.
Https Www Cigna Com Static Www Cigna Com Docs Health Care Providers Form Cms1500 Pdf
APPROVED OMB-093B-1197 FORM CMS-1500 06-15 OMB No.

Printable cms 1500 form. The CMS-1500 form is the standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers DMERCs when a provider qualifies for a waiver from the Administrative Simplification Compliance Act ASCA requirement for electronic submission of claims. It is used to submit a bill or charge for health insurance coverage. The completion of this form is needed to document your voluntary request for termination of Medicare coverage as permitted under the Code of Federal Regulations.
I am looking for a template to complete CSM 1500 health insurance claim forms and print to a standard pre-printed single sheet CMS 1500 red claim. Data elements in the Centers for Medicare Medicaid Services CMS uniform electronic billing specifications are. DO NOT MAIL COMPLETED CLAIM FORMS TO THIS ADDRESS.
T his address is for comments andor suggestions only. Blank Cms 1500 Form Pdf. Locate Client and open Client Profile.
Instructions for Completing OWCP-1500 Health Insurance Claim Form For Medical Services Provided Under the FEDERAL EMPLOYEES COMPENSATION ACT FECA the BLACK LUNG BENEFITS ACT BLBA and the ENERGY EMPLOYEES OCCUPATIONAL ILLNESS. Doctors Initial Report Forms C-4 EC-4 Continuation to CarrierEmployer Billing Section Form C-41 Doctors Progress Report Forms C-42 EC-42 Ancillary Medical Report Forms C-4AMR EC-4AMR. Click Ledger in side menu.
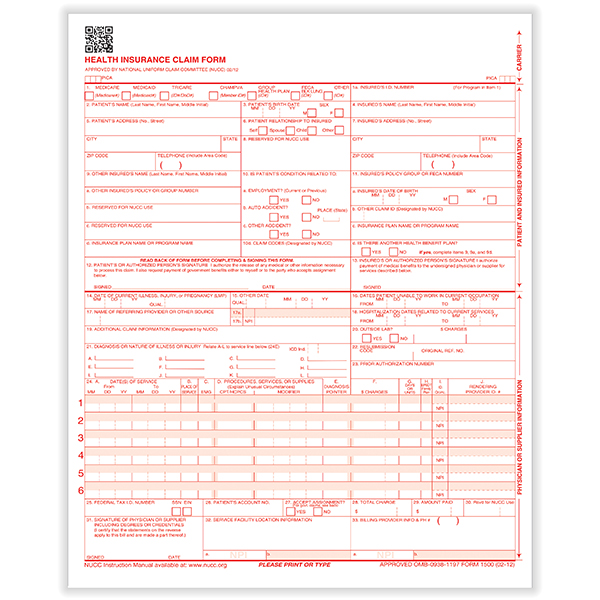
Form CMS-1500 is easy to use and provides all the necessary information when supplemented by a medical narrative. PLEASE PRINT OR TYPE APPROVED OMB-0938-1197 FORM 1500 02-12. 1 Not Required Check Medicaid when billi.
The template could be for MS Word or for MS Excel. Box - include apartment number City State. The Board will replace the following forms with Form CMS-1500.
Claims may be electronically submitted to a Medicare carrier Durable Medical Equipment Medicare Administrative Contractor DMEMAC or AB MAC from a providers office using a computer with software that meets electronic filing requirements as established by the HIPAA claim. Kaiser Permanente requires that all CMS-1500 claims submitted are reported using the specific code sets as adopted by HIPAA. Click Actions and select View Print Blank CMS 1500 for appropriate Invoice.
PLEASE TYPE OR PRINT INFORMATION Form Approved OMB No. Printable Blank Cms 1500 Claim Form. CMS-1500 ZIP Home A.
Professional Paper Claim Form CMS-1500 How to Submit Claims. A HCFA 1500 form is used by the Health Care Financing Administration. Blank Cms 1500 Form Pdf Download.
Cms 1500 Blank Form. 7500 Security Boulevard Baltimore MD 21244. Blank Cms 1500 Form Template.
Printable Blank Cms 1500 Form. Zip code Telephone number. PLEASE PRINT OR TYPE FORM HCFA-1500 12-90 FORM RRB-1500 FORM OWCP-1500 APPROVED OMB-0938-0008.
Item number Required Field. When billing for HMO Copay write or stamp HMO Copay Due in the left top margin. CMS-1500 Template Author.
Form Approved OMB No. Back to PRA Listing. This could be through Medicare Champus group health care or other forms of insurance.
Template for CMS 1500 claim. Health Insurance Common Claims Form. Centers for Medicare Medicaid Services.
Printable Blank Cms 1500 Form. In addition to billing Medicare the 837P and Form CMS-1500 may be suitable for. The code sets for procedures diagnoses and drugs are.
PRA Reports Clearance Officer 7500 Security Boulevard Baltimore Maryland 21244-1850. Detailed information about the medical treatment will be required. Cms-1500 pdf Home A federal government website managed and paid for by the US.
INSUREDS ADDRESS No Street CITY STATE ZIP CODE. I would like to be able to save versions of the file for different patients with their identifying information. Healthcare Common Procedure Coding System HCPCS for ancillary servicesprocedures.
21 Posts Related to Printable Blank Cms 1500 Form. BECAUSE THIS FORM IS USED BY VARIOUS GOVERNMENT AND PRIVATE HEALTH PROGRAMS SEE SEPARATE INSTRUCTIONS ISSUED BY APPLICABLE PROGRAMS. CMS-1500 CMS Form Number.
0521 REQUEST FOR TERMINATION OF PREMIUM HOSPITAL ANDOR SUPPLEMENTARY MEDICAL INSURANCE. Female Street address or PO. Section 1838b and 1818Ac2B of the Social Security Act require.
Claim Form Billing Instructions. Date of Birth mmddyyyy Male. Printable Blank Hcfa 1500 Form.
Free Blank Cms. Research Statistics Data. Current Procedural Terminology CPT-4 for physicians procedures.
Any person who knowingly files a statement of claim containing any. The Form CMS-1500 is the standard paper claim form to bill Medicare Fee-For-Service FFS Contractors when a paper. Regulations.
May 20 2021 by Felix Reiniger. Blank Hcfa 1500 Form. PLEASE PRINT OR TYPE.
Billing various government and some private insurers. It should include the injury or the medical condition that. Accuracy of the time estimates or suggestions for improving this form please write to.
Description and Instructions NA Situational When submitting a Medicare Replacement Plan claim write or stamp Medicare Replacement Plan in the left top margin of the claim. 0938-1197 SECTION 1 - PATIENT INFORMATION Patients Name as shown on Medicare Card Last First Middle Patients Medicare Number exactly as it is shown on the Medicare card. NUMBER For Program in Item 1 4.
PLEASE PRINT OR TYPE APPROVED OMB-0938-1197 FORM 1500 02-12 SA M PL E PLEASE PRINT OR TYPE APPROVED OMB-0938-1197 FORM 1500 02-12 APPROVED OMB-0938-1197 FORM 1500 02-12 1a. It is used for health care claims. CMS-1500 Claim Form.
INSUREDS NAME Last Name First Name Middle Initial 7.
 Amazon Com New Cms 1500 02 12 Claim Form 25 Forms Business Claim Forms Office Products
Amazon Com New Cms 1500 02 12 Claim Form 25 Forms Business Claim Forms Office Products
 Example Of Cms 1500 Form Completed With Cms 1500 Form Free Medical Coding Medical Billing And Coding Medical Billing Training
Example Of Cms 1500 Form Completed With Cms 1500 Form Free Medical Coding Medical Billing And Coding Medical Billing Training
 Claim Forms Fill Out And Sign Printable Pdf Template Signnow
Claim Forms Fill Out And Sign Printable Pdf Template Signnow
 Mental Health Cms1500 Form Download Jpg Pdf
Mental Health Cms1500 Form Download Jpg Pdf
 Hcfa Forms Cms 1500 Medical Forms Health Insurance Claim Forms Formsandchecks Com
Hcfa Forms Cms 1500 Medical Forms Health Insurance Claim Forms Formsandchecks Com
Https Www Cigna Com Static Www Cigna Com Docs Health Care Providers Form Cms1500 Pdf
Blank Cms 1500 Form
 New Cms 1500 Medical Claim Forms Hcfa Approved Version 2012 250 Forms Walmart Com Walmart Com
New Cms 1500 Medical Claim Forms Hcfa Approved Version 2012 250 Forms Walmart Com Walmart Com
 Imprinted Cms 1500 Forms Laser 2500 Pack Justcms1500forms
Imprinted Cms 1500 Forms Laser 2500 Pack Justcms1500forms
 Personalized Cms 1500 Form Personalized Forms
Personalized Cms 1500 Form Personalized Forms
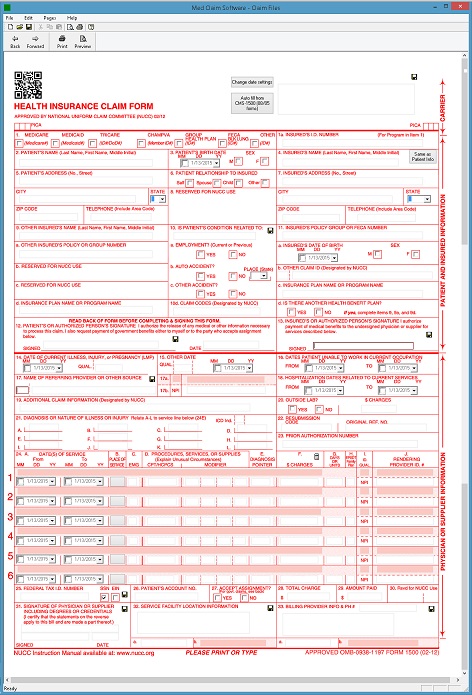
 Hcfa Cms 1500 Medicare Insurance Claim Form Software
Hcfa Cms 1500 Medicare Insurance Claim Form Software
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.