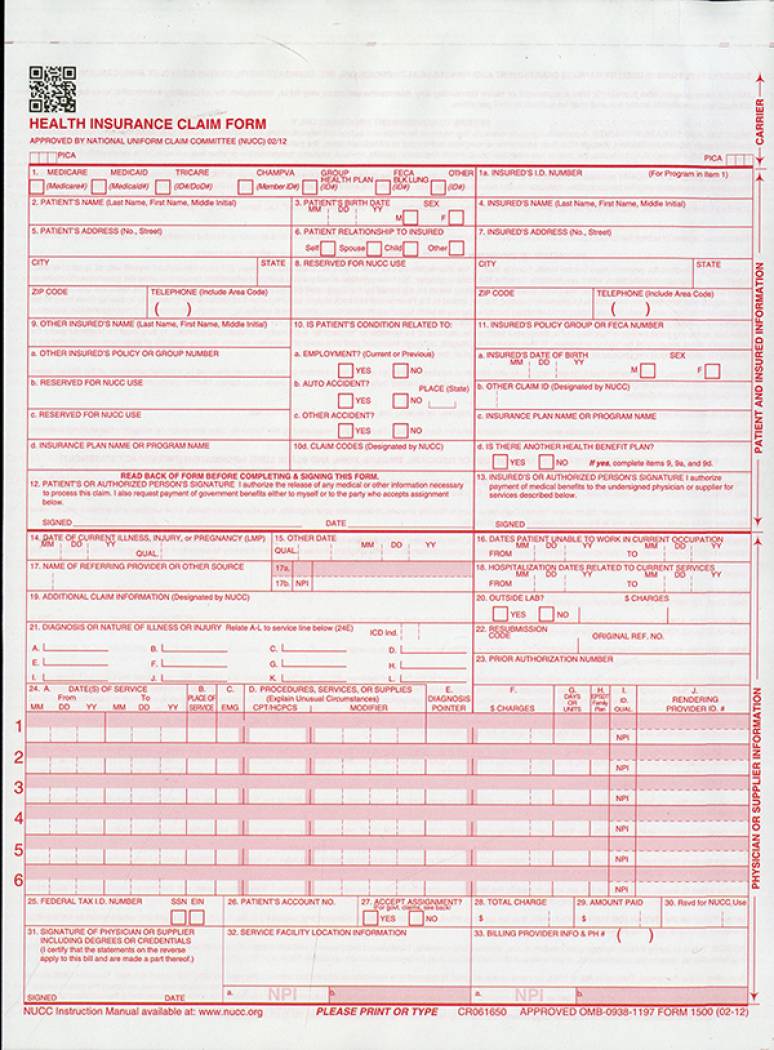
CMS-1500 0212 BILLING INSTRUCTIONS FOR APPLIED BEHAVIORAL ANALYSIS Locator Description Instructions Alerts 1 Medicare Medicaid Tricare Champus Champva Group Health Plan Feca Blk Lung Required -- Enter an X in the box marked MedicaidMedicaid. Instructions for Completing OWCP-1500 Health Insurance Claim Form For Medical Services Provided Under the FEDERAL EMPLOYEES COMPENSATION ACT FECA the BLACK LUNG BENEFITS ACT BLBA and the ENERGY EMPLOYEES OCCUPATIONAL ILLNESS COMPENSATION PROGRAM ACT of 2000 EEOICPA.
 Health Insurance Claim Forms Cms 1500 2 Part Snapout Package Of 100 2012 U S Government Bookstore
Health Insurance Claim Forms Cms 1500 2 Part Snapout Package Of 100 2012 U S Government Bookstore
In Box 28 you will find the total charges for that page of the HCFA 1500.

1500 billing form. The CMS-1500 Form Health Insurance Claim Form is sometimes referred to as the AMA American Medical Association form. This section contains information to help providers bill accurately for physician-administered drugs on the CMS-1500 claim form with a National Drug Code NDC. Please refer to the CMS 1500 Third-Party Liability Claim Instructions or CMS 1500 Medicare Crossover Instructions if applicable.
You must follow these instructions to complete the CMS-1500 claim when billing the Department of Human Services. Any new version of the form must be approved by the White House Office of Management and. It is used for health care claims.
CMS 1500 Billing UPDATED December 20 PAGE 1 CMS 1500 CLAIM INSTRUCTIONS OVERVIEW The following is a block-by-block explanation of how to prepare a CMS 1500 claim form when Medicaid is the primary or only payer. Providers can purchase software from a vendor contract with a billing service or clearinghouse that will provide software or programming support or use HIPAA compliant free billing software that is supplied by Medicare carriers DMEMACs and AB MACs. INSUREDS DATE OF BIRTH b.
2 Required Patients Name. Providers sending professional and supplier claims to Medicare on paper must use Form CMS-1500 in a valid version. Centers for Medicare Medicaid Services.
INSUREDS ADDRESS No Street CITY STATE ZIP CODE TELEPHONE Include Area Code 11. Medicare contractors are allowed to collect a fee to recoup their costs up to 25 if a provider requests a. The form the CMS-1500 throughout this booklet.
Enter the patients date of birth in MMDDCCYY format. It provides information about the client their corresponding insurance policy and their diagnosis and treatment. 1 Not Required Check Medicaid when billing for NM Medicaid services.
1a Required Insureds ID Number. In addition to billing Medicare the 837P and Form CMS-1500 are sometimes suitable for billing various government and some private insurers. 7500 Security Boulevard Baltimore MD 21244.
The CMS-1500 Form is the prescribed form for claims prepared and submitted by physicians or suppliers whether or not the claims are assigned. 3 Required Patients Birth Date. This could be through Medicare Champus group health care or other forms of insurance.
Government Printing Office at 202. NDC Format An NDC number on a drug container consists of digits in a 5-4-2 format. It is used to submit a bill or charge for health insurance coverage.
NUMBER For Program in Item 1 4. Data elements in the CMS uniform electronic billing specifications are. For general policy information refer to the Physician-Administered Drugs.
For questions about the HCFA 1500 claim form or any other form in the billing process please call 507-266-5670. NDC section in this manual. It can be purchased in any version required by calling the US.
INSUREDS NAME Last Name First Name Middle Initial 7. Paper or electronic claim forms must be forwarded to the California Medicaid. Form CMS-1500 is the standard paper claim form used to bill an insurance for rendered services and supplies.
If your claim has multiple pages add the total from each page to figure your total charges for your visit to Mayo Clinic. A HCFA 1500 form is used by the Health Care Financing Administration. APPROVED OMB-0938-1197 FORM 1500 02-12 1a.
September 2020 CMS-1500 Claim Form Description The Health Insurance Claim form CMS-1500 is used by Allied Health professionals physicians laboratories and pharmacies to bill for supplies and services provided to Medi-Cal recipients. Cms-1500 pdf Home A federal government website managed and paid for by the US. Do not imprint type or write any information on the upper.
INSUREDS POLICY GROUP OR FECA NUMBER a. This form is maintained by the National Uniform Claim Committee NUCC an industry organization in which CMS participates. CLAIM ID Designated by.
Enter the patients last name first name and middle initial. Additionally most insurances allow you to send an electronic version called an 837 file. Medicaid Services CMS names the 1500 Health Insurance Claim Form as the CMS-1500 0212 and we call.
Enter the patients NM Medicaid ID number. D CMS-1500 Claim Form 2 Page updated.
