Box 2717 Pittsburgh PA 15230-2717 Attention. You can find detailed instructions on how to file an appeal in the Disputed Claims Process document.
 Carefirst Blue Cross Blue Shield Designation Of Personal Representative Fill Online Printable Fillable Blank Pdffiller
Carefirst Blue Cross Blue Shield Designation Of Personal Representative Fill Online Printable Fillable Blank Pdffiller
2021 Automated Premium Payment ACH Form PDP 2021 Automated Premium Payment ACH Form.
Bcbs authorized representative form. Blue Shield of Michigan on a one-time basis regarding the specific appeal. Evidence of Insurability Medical Evidence of Insurability for coverage changes. BCBSAZ Privacy Office Mail Stop C300 PO.
2021 Access Additional Privacy Forms. Check one Member Grievance and Appeals PO. To have someone else act on your behalf in an appeal complete and return this form.
Just click on a form or document to download it. The member should be the person signing this authorization and designating the release of information. Preferred Drug List PDL Mail Service Registration and Prescription Order Form.
This authorization may be either 1 granted for a particular event or date of service after which time the authorization approval is revoked or 2 granted for any present or future claim for health care benefits you may have. Review Committee Highmark Blue Shield PO. Use this form to designate an authorized representative to speak to Blue Cross on your behalf and to provide access to your information as shown below.
The person listed will be accepted as your authorized representative. If you have medical coverage the following forms and documents are for you. Please read the following for help completing page two of the form.
An authorized representative is not however a person who has legal authority to act on behalf of a member. For ERS or TRS participants refer to specific form links above Form. Life Disability Accident Critical Illness Vision and Dental Enrollment and Change Form You may use this form to enroll in any or all of our group ancillary products.
We are unable to speak with anyone on your behalf unless this form is completed signed and returned to us. Authorization of Representative for purposes of pre- or post-service claim appeal Section 1 Appeal Information Section 2 Patient Information Section 3 Authorized Representative Information I authorize Member Name Authorized Representative Name to act on my behalf to pursue the following appeal of an adverse benefit determination. Authorized Representative Designation Form.
ABA Initial Assessment Request. Use this form to begin the appeals process for Medicare providers. An Authorized Representative is a person you authorize to act on your behalf in pursuing a claim or an appeal of a denied claim.
2021 Authorization to Disclose Protected Health Information PHI Form. Members Authorization Request Form Commercial Operations IDC You may give Blue Cross and Blue Shield of North Carolina Blue Cross NC written authorization to disclose your protected health information PHI to anyone that you designate and for any purpose. Download the forms you need to efficiently administer your ancillary products.
2021 CMS Appointment of Representative Form PDP 2021 CMS Appointment of Representative Form MAPD 2021 CMS Appointment of Representative Form DSNP 2021 Notice of Privacy Practices. Form Title Networks Expedited Pre-service Clinical Appeal Form. Your name Enrollee ID Number Patients name if different from yours Please complete the information to name your authorized representative below.
BLUE CROSS COMMUNITY HEALTH PLANS AUTHORIZED REPRESENTATIVE DESIGNATION. RepresentativeGuardian sectionYou must also provide us with a copy of the legal document showing that you are approved and include it with this form. DESIGNATION OF AUTHORIZED REPRESENTATIVE FOR APPEAL.
Instructions for Filling out the Authorized Representative Form Use the Authorized Representative Form to authorize an individual or organization to pursue an appeal of Blue Cross of Idahos benefit determination on your behalf. Member Authorization Form 109931MUMENABS 918. Mail completed form and Confidential Information Request Form to.
This can be downloaded free of charge at Adobes site. Box 535095 Pittsburgh PA 15253-5095 Attention. Applied Behavior Analysis ABA forms.
This Authorization For Representative Access Form permits you to authorize a billing service service bureau or TPA to have access to designated information for your individual andor group provider codes your Authorized Representative. The Authorized Representative Form also serves as authorization for. Grievance Review Committee Member Grievance and Appeals PO.
Behavioral Health for Other BCBSTX Plans. ABA Clinical Service Request Form. You will need Adobe Reader to view these files.
Use this form to authorize an individual to file an appeal and communicate on your behalf with Blue Cross. Designation of an Authorized Representative To. Medicaid only BCCHP and MMAI.
Medicaid Claims Inquiry or Dispute Request Form. Box 13466 Phoenix AZ 85002-3466. Medicare Level I Appeals Authorization form for appeals on the members behalf Member Appeal Representation Authorization Form New prescription fax order form for PrimeMail Prime Therapeutics - Pharmacy Fax Order Form Form to record your notes from ambulance trips.
Use this form to select an individual or entity to act on your behalf during the disputed claims process. DESIGNATION OF REPRESENTATIVE AS AUTHORIZED REPRESENTATIVE FOR THE DISPUTED CLAIMS PROCESS Name of the Blue Cross and Blue Shield Service Benefit Plan member. Medicaid only BCCHP and MMAI Medicaid Service Authorization Dispute Resolution Request Form.
Use this form to designateremove an individual or entity to act on your behalf as your authorized representative to pursue a benefit claim or. Box 890178 Camp Hill PA 17089-0178 AttentionReview Committee.
 Fillable Online Designation Of Authorized Representative For Appeal Blue Cross Fax Email Print Pdffiller
Fillable Online Designation Of Authorized Representative For Appeal Blue Cross Fax Email Print Pdffiller
Https Www Bluecrossnc Com Document Member Authorization Request Form
 2010 Al Bcbs Form Enr 469 Fill Online Printable Fillable Blank Pdffiller
2010 Al Bcbs Form Enr 469 Fill Online Printable Fillable Blank Pdffiller
Https Www Bcbsm Com Pdf Wf 12077 Authorized Representative And Release Form Pdf
 Form 391 C Designation Of An Authorized Representative Form Highmark Blue Shield Pennsylvania Printable Pdf Download
Form 391 C Designation Of An Authorized Representative Form Highmark Blue Shield Pennsylvania Printable Pdf Download
Https Www Bcbsm Com Content Dam Public Common Documents Grievance Authorization Form Pdf
Https Www Bcbstx Com Pdf Hipaa Hipaa Standard Auth Tx Pdf
Https Www Bcbsm Com Content Dam Public Consumer Documents Help Documents Forms Authorization Use Disclosure Protected Health Information Pdf
Https Www11 Anthem Com Shared Noapplication F5 S2 T0 Pw 041245 Pdf Refer Ahpmember State Va
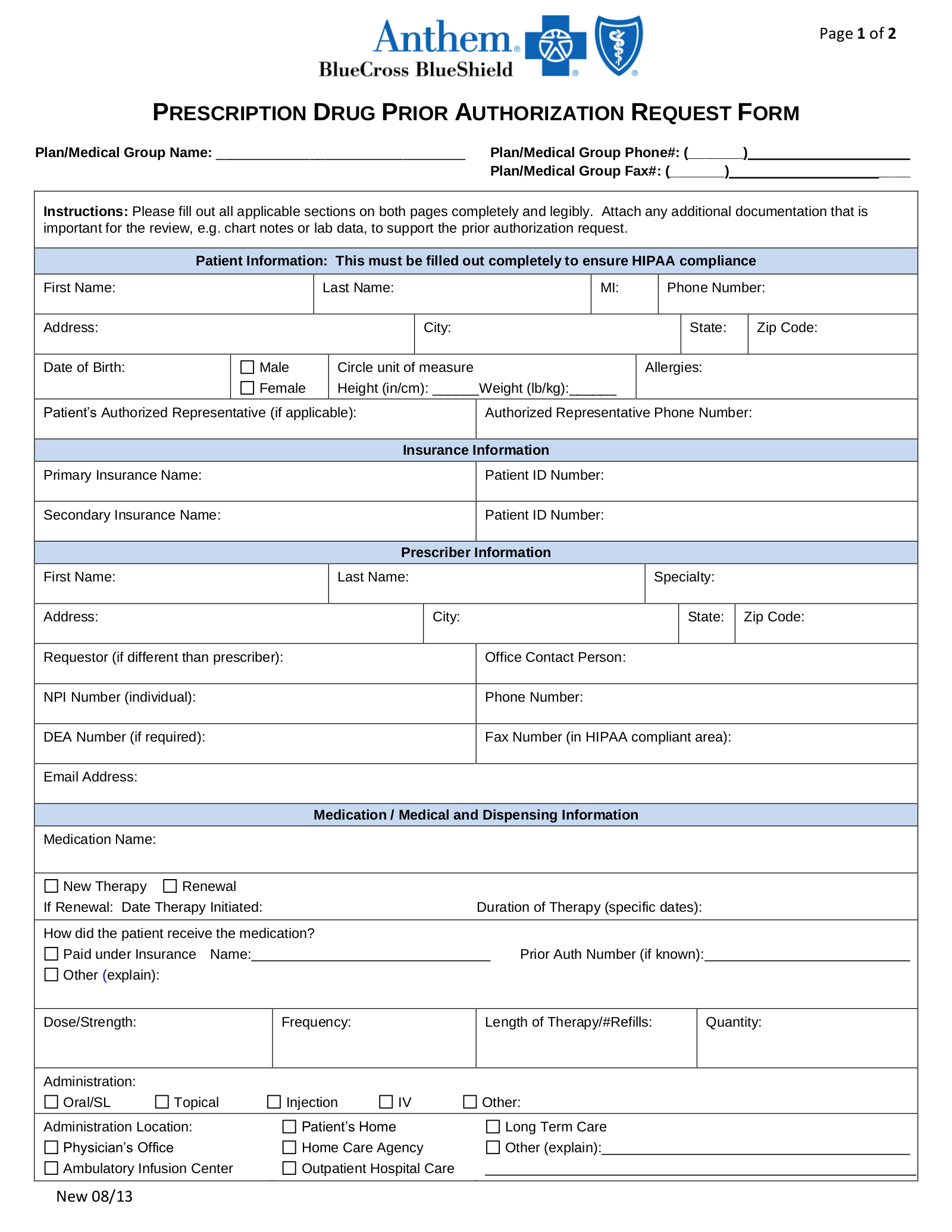 Free Anthem Blue Cross Blue Shield Prior Rx Authorization Form Pdf Eforms
Free Anthem Blue Cross Blue Shield Prior Rx Authorization Form Pdf Eforms
Https Www Bcbsil Com Provider Pdf Forms Standard Authorization Form Pdf
Https Www Anthem Com Health Insurance Nsecurepdf English Common Memauth
Https Www Bcbsmt Com Static Mt Pdf Forms Authorized Representative Form Mt Pdf
Https Www Bluecrossma Org Sites G Files Csphws1866 Files Acquiadam Assets Member S 20designation 20of 20an 20authorized 20representative Pdf
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.