Access all the forms and documents you need to manage your health planfrom claims forms to health information disclosures. Cross and Blue Shield Association.
 Document 12087802
Document 12087802
Out of Network Claim Form.
Blue shield of california reimbursement form. Please forward claims to. Employees who are part of PPO plans that have the Blue Shield Rx Program can use this direct reimbursement form. Employees use this form if the out-of-country provider directly billed Blue Shield of California for covered services.
If you are a Medicare Part D subscriber do not complete this form. Check your Evidence of Coverage EOC or Certificate of Insurance COI to determine if this applies to your plan. Blue Shield of California.
Blue Cross and Blue Shield Companies are independent licensees of the Blue. This materials only plan offers eye wear allowances that supplement the vision plan that is offered by Kaiser. Important instructions Use a separate form A.
877 601-9083 members or 800 877-6372 providers Vision claim form For your protection California law requires the following to appear on this form. You must sign the claim form certification in. BlueCard Worldwide International Claim Form.
If you have filled your prescription at a non-participating pharmacy you can submit a completed claim form along with a detailed receipt. This full service plan offers annual eye exams and eye wear allowances at a variety of providers and retailers. Following the distribution of the notice the California Medical Association CMA received a few calls.
Blue Cross of California is an Independent Licensee of the Blue Cross Association. Search by keywords or filter by category or year to find exactly what youre looking for. Instead visit our website.
SIGNATURE OF SUBSCRIBER. You will be going to a new website operated on behalf of the Blue Cross and Blue Shield Service Benefit Plan by a third party. In a February 6 notice sent to physicians the plan advised that it will be implementing fee schedule changes for durable medical equipment and clinical services.
Out of Network Claim Form. Box 2048 Southeastern PA 19399. Subscriber Claim Form for Services Received Outside California This form is used to submit claims directly to Blue Shield of California or Blue Shield of California Life Health Insurance company when youve received covered services outside of California.
PHYSMETRICS CLAIM FORM PDF This form should be used for outpatient physical therapy occupational therapy speech therapy chiropractic and acupuncture services. Reimbursement will be based on if the medication is covered by Blue Shield and any applicable co-payment co-insurance percentage co-payment. Please see the instructions on the reverse side of this form before completing.
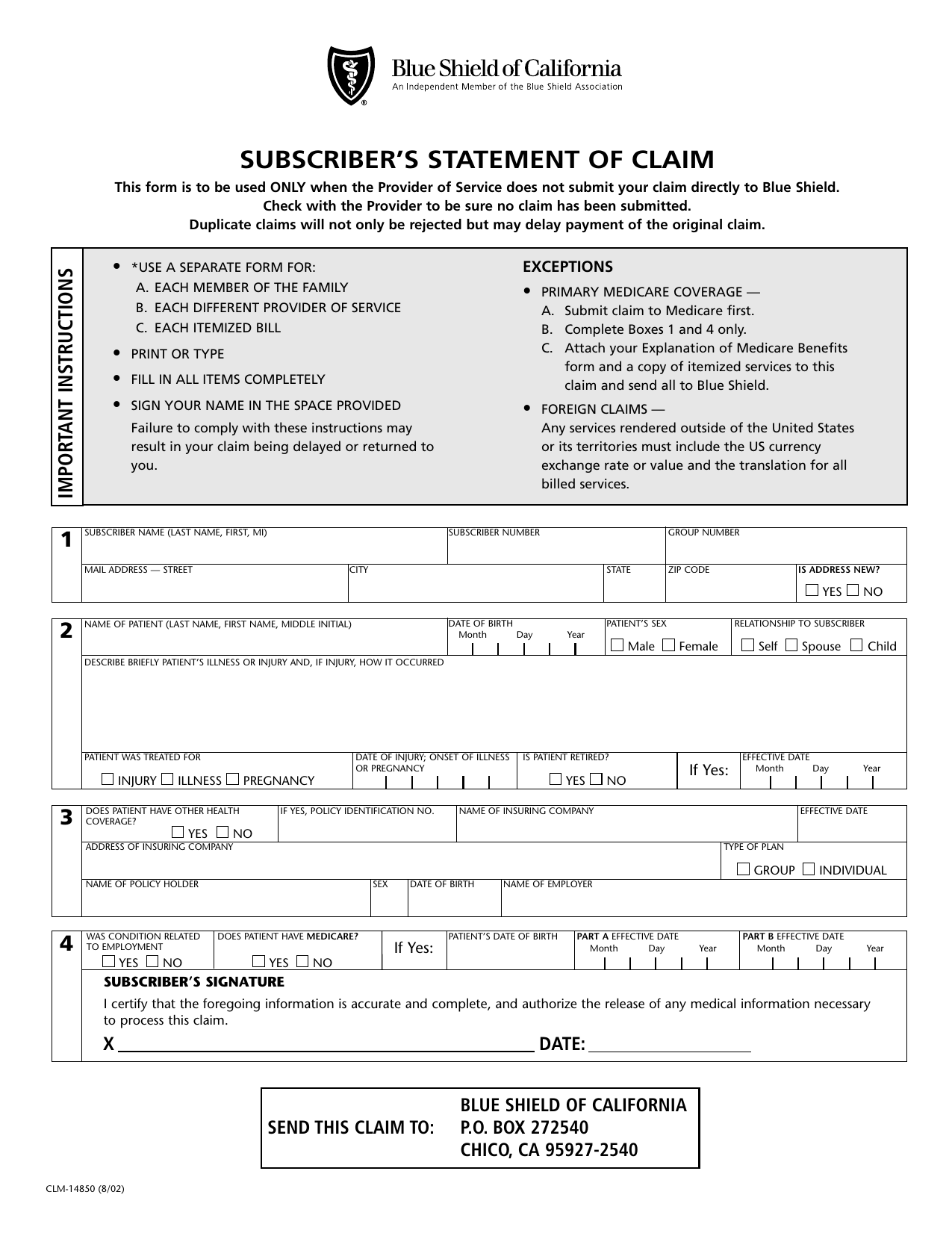
Blue Shield of California PO. Duplicate claims will not only be rejected but may delay payment of the original claim. Blue Shield of California Prescription Drug Reimbursement form Also applies to outpatient prescription drug benefits available through plans underwritten by Blue Shield of California Life Health Insurance Company.
Send completed form and documentation to. You should only use this form when you are certain that the provider of service has not and will not submit a claim for you. I authorize the release of any medical information necessary to process this claim.
Find forms and documents. Overseas members should use the Overseas Medical Claim Form. Kaiser Permanente MES Vision Plan.
Blue Shield of California Prescription Drug Benefit Direct Reimbursement Claim Applies to outpatient prescription drug benefits available through plans underwritten by Blue Shield of California Life Health Insurance Company. Any person who knowingly presents a false or fraudulent claim for payment of a loss is guilty of a crime. The protection of.
Download PDF PDF 110KB Blue Shield of California Prescription Drug Benefit - Direct Reimbursement Claim. Instructions Please wait until you receive your Blue Shield ID card before sending this claim for reimbursement. Blue Cross Blue Shield Settlement CO JND Legal Administration PO Box 91390 Seattle WA 98111 9.
C-14352 0103 - April 12 2007 A n I n d e p e n d e n t M e m b e r o f t h e B l u e. CONTINUITY OF CARE FORM - This form is used by new and current members of a Blue Shield of California plan to request continuity of care services. If you use a provider outside of the network you will need to complete and file a claim form for reimbursement.
Box 25208 Santa Ana CA 92799-5208. Blue Shield MES Vision Plan. Our mission and values are embodied in our proposal to guarantee health coverage for all Californians the first time a major health plan has called for.
I certify that the information on this Member Claim Form is true and correct to the best of my knowledge. And mail it to the address below postmarked by _____ in order for your claim to be considered. Blue Shield of California has announced upcoming changes to its physician fee schedule that will take effect on April 15 2020.
As a not-for-profit health plan Blue Shield is guided by our mission and values which encourage innovation and enable us to be a catalyst for constructive change. Subscribers Statement of Claim This form is to be used ONLY when the Provider of Service does not submit your claim directly to Blue Shield. This Member Claim Form was developed to notify Blue Shield of California of any covered health service for which they have not already been billed.
Check with the Provider to be sure no claim has been submitted.
Https Www Blueshieldca Com Sites Uc Documents Claim Form Ca Lm15481 Ff Pdf
 Fillable Online Accelerated Death Benefit Claim Form For Blue Shield Superagent Fax Email Print Pdffiller
Fillable Online Accelerated Death Benefit Claim Form For Blue Shield Superagent Fax Email Print Pdffiller
 Fillable Online Countyofsb Subscriber Statement Form Fax Email Print Pdffiller
Fillable Online Countyofsb Subscriber Statement Form Fax Email Print Pdffiller
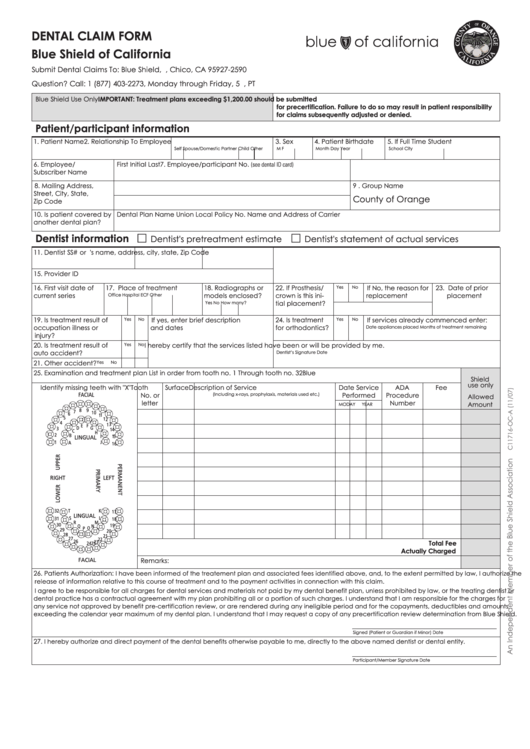 Dental Claim Form Blue Shield Of California Printable Pdf Download
Dental Claim Form Blue Shield Of California Printable Pdf Download
Https Www Blueshieldca Com Bsca Bsc Public Common Portalcomponents Sites Streamdocumentservlet Filename Bsp 2019 Provider 20dispute 20resolution 20request Pdf
2
Https Www Smgov Net Uploadedfiles Departments Hr Benefits 2019 20rx 20reimbersement 20form Pdf
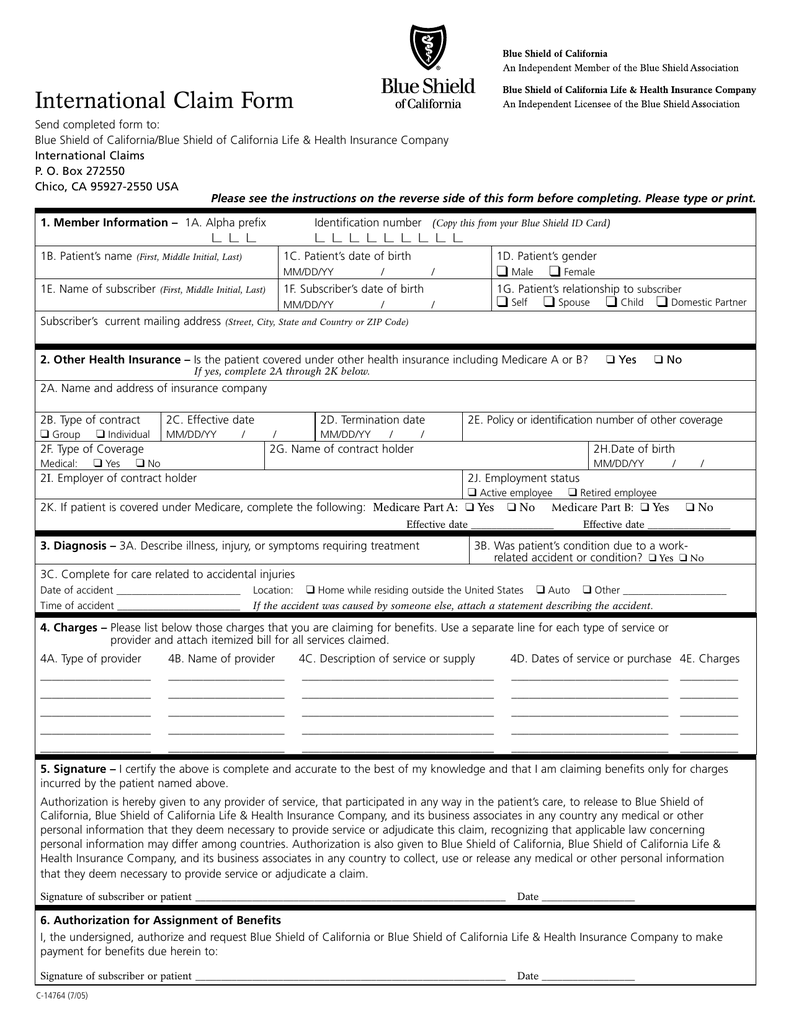 International Claim Form
International Claim Form
Https Www Blueshieldca Com Bsca Bsc Public Broker Portalcomponents Streamdocumentservlet Filename C4669 61 Ff Pdf
Https Www Blueshieldca Com Sites Stanford Documents Prescription Drug Reimbursement Claim Form 4 7 Pdf
 Fillable Online Vision Claim Form Blue Shield Of California And Blue Shield Of Fax Email Print Pdffiller
Fillable Online Vision Claim Form Blue Shield Of California And Blue Shield Of Fax Email Print Pdffiller
 Fillable Online Medical Claim Form Blue Shield Fax Email Print Pdffiller
Fillable Online Medical Claim Form Blue Shield Fax Email Print Pdffiller
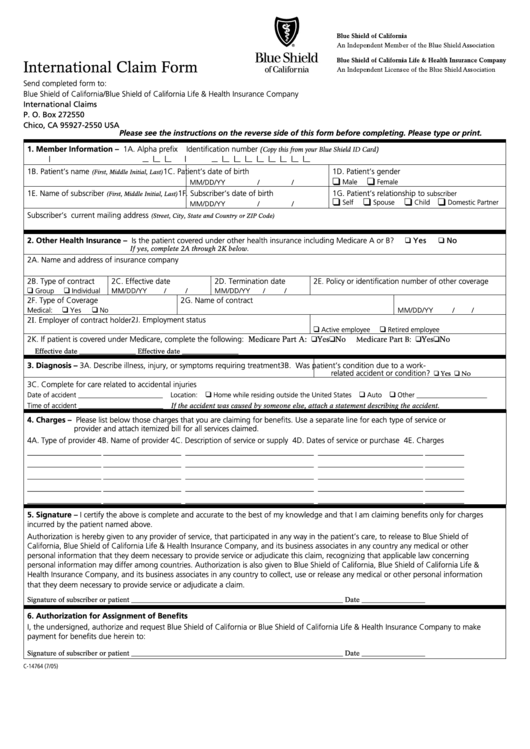 Form C 14764 International Claim Form Blue Shield Of California Printable Pdf Download
Form C 14764 International Claim Form Blue Shield Of California Printable Pdf Download
 Fillable Online Blue Shield Of California Provider Identification Number Application Form Fax Email Print Pdffiller
Fillable Online Blue Shield Of California Provider Identification Number Application Form Fax Email Print Pdffiller
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.